Oxygen-Regulation of Erythropoiesis and Iron Metabolism
The Haase Lab studies oxygen-regulation of erythropoiesis and iron metabolism with a focus on the mechanisms that lead to the development of anemia associated with chronic kidney disease (CKD), also known as renal anemia. Major contributing factors to the development of anemia in patients with CKD are relative erythropoietin (EPO) deficiency, ie., the impaired ability of the diseased kidney to produce EPO, absolute and/or functional iron deficiency, resistance to EPO signaling and reduced life span of red blood cells. (click here for a detailed review on renal anemia)
(click on image to enlarge)
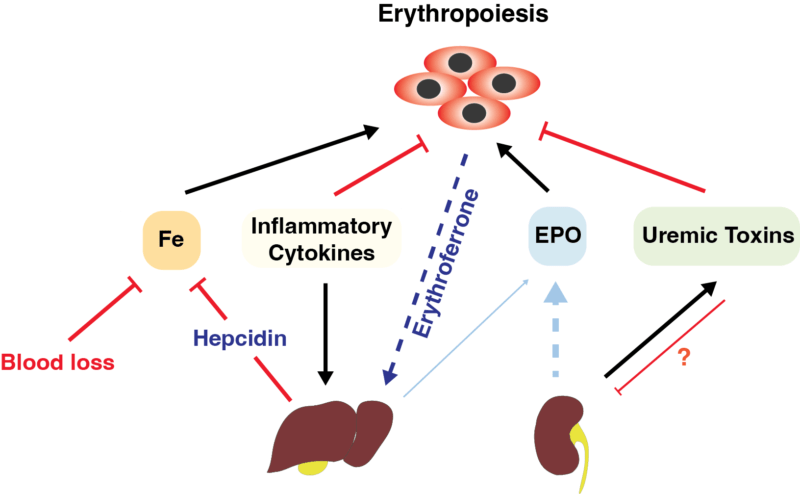
Mechanisms of renal anemia. Shown is an overview of factors and conditions that contribute to the pathogeneis of renal anemia. The impaired ability of the kidney to produce EPO is indicated by a dashed line. Inflammatory cytokines suppress erythropoiesis in the BM and stimulate hepcidin production in the liver, which impacts iron absorption and mobilization negatively. Hepcidin is also maintained at higher levels by decreased errythroferrone production (dotted blue line), which is secondary to a reduction in erythroblast numbers due to EPO deficiency in renal failure. In patients with advanced CKD, the liver contributes significantly to serum EPO levels. The contribution of uremic toxins to the pathogenesis of renal anemia is only poorly understood. Uremic toxins have been shown to suppress erythroid colony formation in vitro as well as EPO transcription in hepatoma cells, the latter indicating possible suppressive effects on hepatic and renal EPO production in vivo (indicated by red line).
Over the last decade the Haase group has focused on investigating the role of HIF in the regulation of erythropoiesis and iron metabolism. We have generated multiple genetic models of anemia and polycythemia and have contributed to the development of drugs that are currently in clinical development for renal anemia (HIF stabilizers). Specifically, we have identified HIF-2 as the key regulator of renal EPO synthesis and have established that HIF coordinates erythropoiesis with iron metabolism by directly regulating iron uptake and release.
More recently, the Haase lab investigated the role of HIF in the regulation of hepcidin and was able to show that the hypoxic suppression of hepcidin occurs indirectly through HIF-2-mediated stimulation of erythropoiesis. We have now developed novel genetic models to further dissect the PHD/HIF axis in various renal cell populations and have begun to interrogate the hypoxic regulation of HIF-2 signaling in renal interstitial cells under physiologic and injury conditions.
(click on image to enlarge)
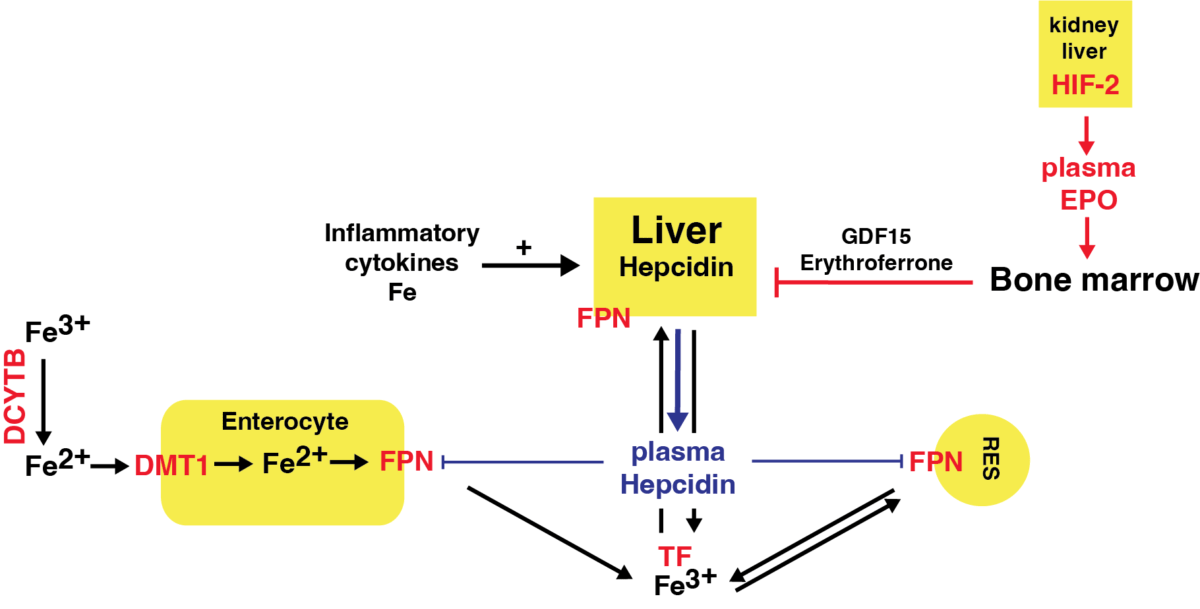
HIF-dependent regulation of iron metabolism. Schematic overview of HIF-regulated genes involved in iron metabolism shown in red. In the gut duodenal cytochrome b (DCYTB) reduces ferric iron (Fe3+) to its Fe2+, which enters enterocytes via the divalent metal transporter-1 (DMT1). DCYTB and DMT1 are both bona fide HIF-2-regulated genes. Release of iron into the circulation occurs via ferroportin (FPN), which is hepcidin-regulated but also HIF-inducible. In blood, iron is transported in complex with transferrin (TF) to the liver, cells of the reticulo-endothelial system (RES), bone marrow and other organs. Increased erythropoietic activity in the BM produces growth differentiation factor 15 (GDF15) and erythroferrone, which have been shown suppress hepcidin in hepatocytes. Inflammatory cytokines stimulate hepcidin production in the liver and lead to reduced ferroportin surface expression and hypoferremia.
Relevant Publications from the Haase Lab
- Kobayashi H, Davidoff O, Pujari-Palmer S, Drevin M, Haase VH. EPO synthesis induced by HIF-PHD inhibition is dependent on myofibroblast transdifferentiation and colocalizes with non-injured nephron segments in murine kidney fibrosis. Acta Physiol (Oxf) [print-electronic]. 2022 May 5/1/2022; e13826. PMID: 35491502.
- Haase VH. Hypoxia-inducible factor-prolyl hydroxylase inhibitors in the treatment of anemia of chronic kidney disease. Kidney Int Suppl (2011) [print-electronic]. 2021 Apr; 11(1): 8-25. PubMed PMID: 33777492.
- Burmakin M, Fasching A, Kobayashi H, Urrutia AA, Damdimopoulos A, Palm F, Haase VH. Pharmacologic HIF-PHD inhibition reduces renovascular resistance and increases glomerular filtration by stimulating nitric oxide generation. Acta Physiol (Oxf) [print-electronic]. 2021 Apr 4/26/2021; e13668. PMID: 33900001. See associated commentary: “Get used to the -dustats: Roxadustat and molidustat, members of the hypoxia-inducible factor (HIF) Prolyl hydroxylase (PHD) inhibitor drug class promote kidney function, perfusion and oxygenation in rats through nitric oxide”; [Acta Physiologica 2021].
- Sanghani NS, Haase VH. Hypoxia-Inducible Factor Activators in Renal Anemia: Current Clinical Experience. Adv Chronic Kidney Dis. 2019 Jul;26(4):253-66. PMID: 31477256.
- Pergola PE, Spinowitz BS, Hartman CS, Maroni BJ, Haase VH. Vadadustat, a novel oral HIF stabilizer, provides effective anemia treatment in nondialysis-dependent chronic kidney disease. Kidney Int [print-electronic]. 2016 Nov; 90(5): 1115-22. PMID: 27650732. See associated commentary: “HIF stabilization by prolyl prolyl hydroxylase inhibitors for the treatment of anemia in chronic kidney disease“.
- Urrutia AA, Afzal A, Nelson J, Davidoff O, Gross KW, Haase VH. Prolyl-4-hydroxylase 2 and 3 coregulate murine erythropoietin in brain pericytes. Blood. 2016 Nov 11/24/2016; 128(21): 2550-60. PMID: 27683416. See associated commentary in the same issue of Blood: “Pericytes: new EPO-producing cells in the brain”.
- Kobayashi H, Liu Q, Binns TC, Urrutia AA, Davidoff O, Kapitsinou PP, Pfaff AS, Olauson H, Wernerson A, Fogo AB, Fong GH, Gross KW, Haase VH. Distinct subpopulations of FOXD1 stroma-derived cells regulate renal erythropoietin. J Clin Invest. 2016 May 2;126(5):1926-38. PubMed PMID: 27088801.
- Farsijani NM, Liu Q, Kobayashi H, Davidoff O, Sha F, Fandrey J, Ikizler TA, O’Connor PM, Haase VH. Renal epithelium regulates erythropoiesis via HIF-dependent suppression of erythropoietin. J Clin Invest. 2016 Apr 1;126(4):1425-37. PubMed PMID: 26927670. See associated commentary in Nature Reviews Nephrology: “Regulation of renal erythropoietin via HIF“.
- Liu Q, Davidoff O, Niss K, Haase VH. Hypoxia-inducible factor regulates hepcidin via erythropoietin-induced erythropoiesis. J Clin Invest. 2012 Dec;122(12):4635-44. PubMed PMID: 23114598.
- Kapitsinou PP, Liu Q, Unger TL, Rha J, Davidoff O, Keith B, Epstein JA, Moores SL, Erickson-Miller CL, Haase VH. Hepatic HIF-2 regulates erythropoietic responses to hypoxia in renal anemia. Blood [print-electronic]. 2010 Oct 10/21/2010; 116(16): 3039-48. PubMed PMID: 20628150. See associated commentary in the same issue of Blood: “Dual control: the HIF-2 regulator“.
- Rankin EB, Biju MP, Liu Q, Unger TL, Rha J, Johnson RS, Simon MC, Keith B, Haase VH. Hypoxia-inducible factor-2 (HIF-2) regulates hepatic erythropoietin in vivo. J Clin Invest. 2007 Apr;117(4):1068-77. PubMed PMID: 17404621. See associated commentary in the same issue of JCI: “HIF-1 and HIF-2: working alone or together in hypoxia?“